Estimates for the decrease in recurrent VTE, increase in major bleeding, and associated deaths with 5 years of extended anticoagulation vs no anticoagulation in patients with different combinations of recurrent VTE and bleeding risk
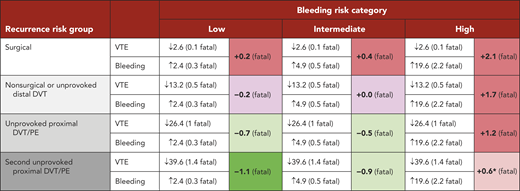
Color coded cells show the estimated net difference in deaths due to VTE and major bleeding. With the ACCP recommendations, for extended anticoagulation, dark green indicates a strong recommendation in favor (>1 lives saved over 5 y), light green indicates a weak recommendation in favor (0.5 to 1.0 lives saved over 5 y), light red indicates a weak recommendation against (0 to 0.5 lives saved over 5 y) and dark red indicates a strong recommendation against (lives lost over 5 y).
Despite an average estimated increase of +0.6 deaths, a weak recommendation against extended therapy is provided in recognition that the bleeding risk will be lower than the average value in many patients.
Assumptions:
Percentage risk for recurrent VTE without anticoagulation (after 1 and 5 years) in patients with: first VTE provoked by surgery (1%, 3%); first VTE provoked by nonsurgical factor or unprovoked isolated distal DVT (5%, 15%); unprovoked proximal DVT or PE (10%, 30%); 2nd episode of unprovoked VTE (15%, 45%).
Case fatality proportion for an episode of recurrent VTE after stopping anticoagulation: 3.6%.
Reduction in recurrent VTE with anticoagulation: 88%.
Percentage risk for major bleeding without anticoagulation (annual, not including within 3 mo of VTE diagnosis): low (0.3%); moderate (0.6%); high (≥2.5%, acknowledging that there is a broad range of risks within this subgroup). See ”Influence of bleeding risk on the decision to anticoagulate indefinitely.”
Increase in major bleeding with anticoagulation: 2.6 fold risk or a 160% increase. Assuming that use of a DOAC would be associated with two-thirds the risk of major bleeding would only change one recommendation for extended anticoagulation; strong in favor instead of weak in favor for patients with a second unprovoked VTE who had a moderate risk of bleeding.
Case fatality proportion for an episode of major bleeding: 11.3%.